By David Gans · May 4, 2026

How multivitamins improve recovery after bariatric surgery
If you just had bariatric surgery and someone handed you a standard one-a-day multivitamin from the drugstore shelf, that’s a problem. Most post-op patients don’t realize that lifelong micronutrient supplementation is a clinical requirement after surgery, not just a general wellness suggestion. Your anatomy has changed, your absorption has changed, and your nutritional needs have changed in ways that a generic multivitamin simply cannot address. This guide breaks down exactly why bariatric-specific multivitamins matter, what they contain, and how to use them to support a stronger, safer recovery.
Table of Contents
- Why recovery after bariatric surgery demands more than standard vitamins
- What’s in a bariatric multivitamin? Nutrients and daily targets explained
- Bariatric-specific vs. standard multivitamins: What does the evidence say?
- How to use multivitamins for optimal recovery: Pro tips, timing, and troubleshooting
- Our take: Most patients and some providers underestimate the lifelong role of multivitamins
- Find the best bariatric multivitamins for your recovery
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Lifelong nutrient support | After bariatric surgery, specialized multivitamins are essential to prevent serious vitamin and mineral deficiencies. |
| Bariatric formulas are critical | Standard multivitamins often lack the dosage and forms needed for effective recovery in bariatric patients. |
| Personalized regimens matter | Your surgery type and health status determine dosing. Work with your care team for optimal results. |
| Routine monitoring | Lab checks and clinical follow-up are key to ensuring your supplement plan is working. |
Why recovery after bariatric surgery demands more than standard vitamins
To understand why specialized multivitamins matter, we need to look at how your body’s needs change after surgery.
Bariatric procedures like Roux-en-Y gastric bypass (RYGB), gastric sleeve, and mini-bypass all reduce the functional size of your stomach and, in bypass procedures, reroute the digestive tract. This means less food intake and, critically, less surface area available to absorb nutrients. The result is a body that is working hard to heal from major surgery while simultaneously struggling to pull in the vitamins and minerals it needs.
The risks of bariatric vitamin deficiencies are not theoretical. Left unaddressed, micronutrient gaps can lead to serious clinical conditions:
- Iron deficiency anemia: Particularly common in menstruating women after RYGB, due to reduced acid production and bypassed absorptive segments.
- Bone disease (osteoporosis/osteomalacia): Calcium and vitamin D malabsorption accelerates bone loss over time.
- Neurologic complications: Thiamine (vitamin B1) and vitamin B12 deficiencies can cause peripheral neuropathy, memory problems, and in severe cases, irreversible nerve damage.
- Zinc and copper imbalances: Both affect immune function, wound healing, and hair health, which is why hair loss is so common in the first year post-op.
“In bariatric patients, multivitamins play a structural role similar to nutrient replacement therapy. Reduced intake and malabsorption increase the risk of anemia, bone disease, and neurologic complications unless micronutrient targets are consistently met.”
Standard over-the-counter multivitamins are formulated for the general population, people with intact digestive anatomy who eat a full diet. They simply do not contain the doses or the specific nutrient forms required to compensate for post-op malabsorption. Taking one anyway is not just insufficient. It can create a false sense of security while deficiencies quietly develop.

What’s in a bariatric multivitamin? Nutrients and daily targets explained
With these risks in mind, let’s look at exactly what makes a bariatric-specific multivitamin and how its contents differ from typical supermarket options.
Bariatric multivitamins are formulated to hit elevated micronutrient targets that align with ASMBS (American Society for Metabolic and Bariatric Surgery) guidelines. The micronutrient dosing framework is procedure-specific, meaning what you need after RYGB differs meaningfully from what you need after a sleeve gastrectomy.
Here is a breakdown of core nutrients and why each one matters:
- Thiamine (B1): Critical for nerve function and energy metabolism. Deficiency can develop within weeks post-op and is one of the most urgent nutritional risks.
- Folate (B9): Needed for cell production and DNA repair. Especially important for women of childbearing age.
- Vitamin B12: Absorption depends on intrinsic factor, which is reduced after RYGB. Sublingual or methylcobalamin forms are often better tolerated than standard cyanocobalamin tablets.
- Iron: Absorbed primarily in the duodenum, which is bypassed in RYGB. Ferrous bisglycinate is a gentler, more bioavailable form than ferrous sulfate.
- Vitamin D3: Fat-soluble and dependent on bile acids for absorption. Most post-op patients need 3,000 IU or more daily to maintain adequate 25-OH vitamin D levels.
- Calcium citrate: Unlike calcium carbonate, calcium citrate does not require stomach acid for absorption, making it the only appropriate form after bariatric surgery.
- Zinc and copper: Must be balanced carefully. High zinc supplementation without copper can cause copper deficiency anemia.
- Vitamins A, E, and K: Fat-soluble vitamins that can become depleted, particularly after malabsorptive procedures.
Daily targets by procedure type
| Nutrient | RYGB | Gastric sleeve | Mini-bypass |
|---|---|---|---|
| Vitamin B12 | 350-500 mcg/day (oral) | 350-500 mcg/day | 350-500 mcg/day |
| Iron | 45-60 mg/day (menstruating women: up to 80-100 mg) | 18-45 mg/day | 45-60 mg/day |
| Calcium citrate | 1,200-1,500 mg/day (divided doses) | 1,200-1,500 mg/day | 1,200-1,500 mg/day |
| Vitamin D3 | 3,000 IU/day minimum | 3,000 IU/day | 3,000 IU/day |
| Thiamine | 12 mg/day minimum | 12 mg/day | 12 mg/day |
| Zinc | 8-22 mg/day | 8-22 mg/day | 8-22 mg/day |
For patients who have had a sleeve gastrectomy, the malabsorptive risk is lower than with bypass, but the restrictive nature of the surgery still limits dietary intake significantly. For those who had gastric bypass, both restriction and malabsorption are in play, which is why iron and B12 targets are especially critical.
Pro Tip: If you are a menstruating woman post-RYGB, your iron needs can be nearly double the standard recommendation. Look specifically for bariatric multivitamins that include at least 45 mg of iron per serving, and confirm with your provider whether you need a separate iron supplement on top of that.
Bariatric-specific vs. standard multivitamins: What does the evidence say?
Now that we know what’s in a bariatric multivitamin, let’s see how these formulations stack up against traditional options when it comes to real-life recovery.
The clinical evidence is clear on one point: standard multivitamins consistently fall short for post-bariatric patients. A key study published in the journal Medicine found that bariatric-specific multivitamins improved outcomes for iron and vitamin B12 deficiency in RYGB populations compared to standard supplementation regimens. The same pattern holds for vitamin D, where post-op patients on standard multivitamins frequently fail to maintain adequate serum 25-OH vitamin D levels above 30 ng/mL.
Researchers evaluating recovery study designs have noted that meaningful comparisons require tracking biochemical markers like ferritin, serum B12, and 25-OH vitamin D over time, not just asking whether patients took a vitamin. When those markers are tracked, the gap between bariatric-formulated and standard products becomes very apparent.
Deficiency rates: Bariatric-specific vs. standard multivitamins
| Nutrient | Deficiency rate with standard MVI | Deficiency rate with bariatric MVI |
|---|---|---|
| Iron (RYGB) | Up to 49% at 1-2 years post-op | Significantly reduced with procedure-specific dosing |
| Vitamin B12 | Up to 30-40% without supplementation | Reduced with sublingual or high-dose oral B12 |
| Vitamin D | Up to 60-70% insufficient at 12 months | Improved with D3 at 3,000+ IU/day |
| Thiamine | Risk highest in first 3 months post-op | Mitigated with adequate B1 in bariatric formula |
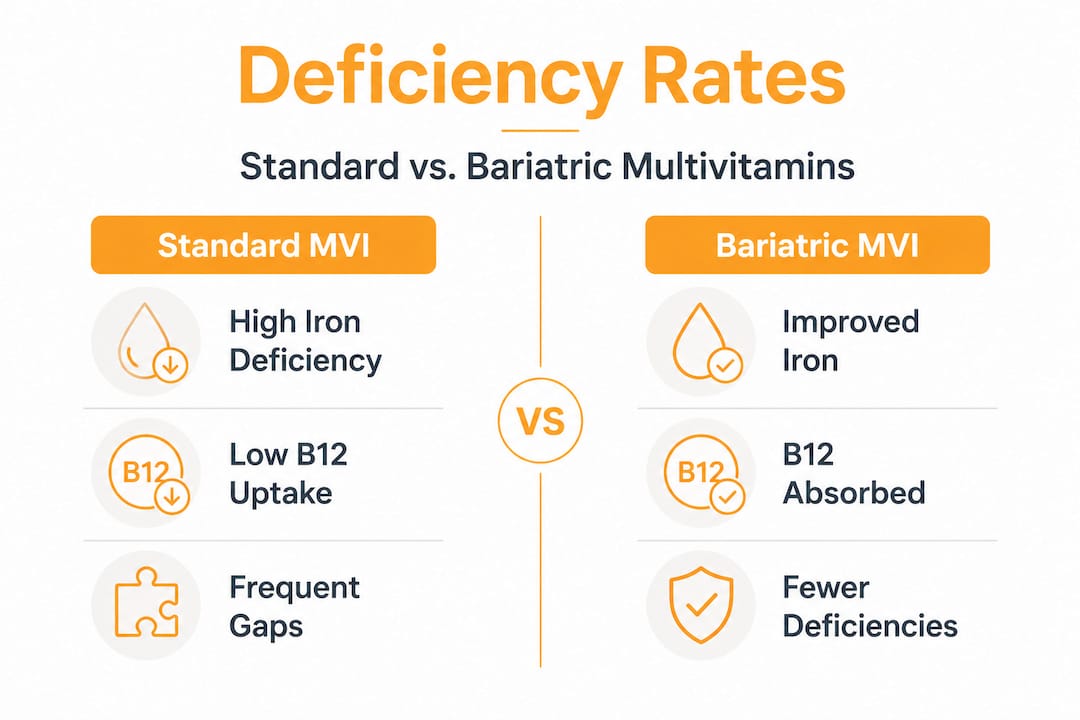
The difference isn’t just about higher doses. It’s also about nutrient form. A standard multivitamin might include cyanocobalamin for B12 and calcium carbonate for calcium. Neither works well after bariatric surgery. Bariatric formulas use methylcobalamin and calcium citrate for a reason. Those forms are absorbed without the gastric acid and intrinsic factor that your post-op body can no longer reliably produce.
Understanding how needs differ between procedures is also important here. RYGB patients face higher malabsorption risk across the board, while sleeve patients face primarily restrictive challenges. That distinction matters when choosing a formula and when preventing B12 deficiency specifically.
How to use multivitamins for optimal recovery: Pro tips, timing, and troubleshooting
Armed with the science, let’s make sure you’re using bariatric multivitamins to their full recovery potential.
Getting the right product is step one. Using it correctly is step two, and it’s where a lot of patients fall short. Here is a practical, step-by-step approach:
-
Start at the right time. Most bariatric programs recommend beginning chewable or liquid vitamins within the first few days post-op, before you can tolerate capsules. If you’re unsure about when to start supplements, your surgical team should provide a specific timeline.
-
Choose the right form for your stage. Chewables and dissolvables are ideal in the first 4-6 weeks. Capsules are fine once you can tolerate solid foods. Avoid large tablets early on.
-
Separate calcium and iron. This is one of the most important rules and one of the most commonly ignored. Calcium and iron compete for the same absorption pathways, so taking them together dramatically reduces how much of each you actually absorb. Space them at least 2 hours apart. Calcium citrate should be taken in divided doses of 500-600 mg at a time, never all at once.
-
Take fat-soluble vitamins with a meal. Vitamins A, D, E, and K are absorbed better when consumed alongside a small amount of dietary fat. Even a few bites of food with healthy fat is enough.
-
Monitor your labs consistently. Blood work every 3-6 months in the first year, then annually, is the standard of care. Key markers include ferritin (not just hemoglobin), serum B12, 25-OH vitamin D, zinc, copper, and a complete metabolic panel.
-
Don’t ignore symptoms. Fatigue, hair loss, tingling in the hands or feet, and brain fog are not just “part of recovery.” They are potential signs of deficiency. Don’t wait for your next scheduled lab if these symptoms appear.
Common pitfalls to avoid:
- Staying on a standard OTC multivitamin because it’s cheaper or more convenient
- Taking all supplements at once to simplify your routine (especially calcium and iron together)
- Stopping vitamins once you feel better, assuming your body has “caught up”
- Skipping labs because you feel fine
Per ASMBS-aligned clinical guidance, deficiencies and nutrient interactions can persist or develop despite supplementation. Clinicians typically tailor formulations, modify timing, and escalate to injections or alternate routes when oral absorption or tolerance is inadequate.
Pro Tip: If you are experiencing GI intolerance with your current multivitamin, don’t just stop taking it. Talk to your bariatric dietitian about switching forms or brands. There are significant differences between products in terms of tolerability, and finding the right one is worth the effort.
Our take: Most patients and some providers underestimate the lifelong role of multivitamins
I am David Gans. I lost 231 lbs after gastric bypass in January 2024, and I can tell you from personal experience that “just take a multivitamin” is advice that sounds simple but hides a lot of complexity.
In the first few months post-op, I was doing everything right on paper. I was taking a multivitamin every day. What I didn’t know was that I was taking the wrong one. It wasn’t until my six-month labs came back with low ferritin and borderline B12 that my dietitian pointed out I needed a bariatric-specific formula with higher iron and sublingual B12. That was a wake-up call.
Here’s the uncomfortable truth: a lot of patients are winging it with their supplements. And some providers, particularly those who aren’t bariatric specialists, don’t push hard enough on the specifics. I’ve heard from many people in bariatric communities who were told “just take a Centrum” by a well-meaning but non-specialist physician. That guidance, while not malicious, can lead to real deficiencies down the road.
The evidence-based guidance is clear: if a patient cannot meet bariatric micronutrient targets with a standard OTC multivitamin, procedure-specific bariatric formulas are the appropriate solution. This isn’t optional. It’s the standard of care.
What I always tell people is this: your multivitamin regimen is not a set-it-and-forget-it situation. It needs to evolve as your body changes, as your labs change, and as you transition from early recovery to long-term maintenance. Explore the detailed vitamin guides on this site to stay informed at every stage.
Find the best bariatric multivitamins for your recovery
If you’re ready to take the next informed step, these resources can help you recover with confidence.
Choosing the right bariatric multivitamin doesn’t have to be overwhelming. At BestBariatricMultivitamins.com, we’ve done the research so you don’t have to start from scratch.
We compare bariatric multivitamin options across 15 manufacturer-labeled products, evaluating price per day, iron content, form (capsule, chewable, dissolvable), and surgery type fit. Whether you’ve had gastric bypass, sleeve, or mini-bypass, there’s a product comparison built for your specific needs. If you want to understand what to watch for before deficiencies become a problem, our guide on vitamin deficiency signs is a practical place to start. Your recovery deserves more than guesswork.
Frequently asked questions
Why can’t I just take a standard one-a-day multivitamin after bariatric surgery?
Standard multivitamins don’t provide the doses or the specific nutrient forms required after bariatric procedures. The procedure-specific dosing framework for iron, fat-soluble vitamins, and B12 far exceeds what a typical OTC product contains.
What happens if I skip my bariatric multivitamin for a few weeks?
Even a few weeks without supplementation can allow deficiencies to develop or worsen, increasing your risk of anemia, bone disease, and neurologic complications given the ongoing malabsorption that persists long after surgery.
Do I need to separate my calcium and iron supplements?
Yes. Calcium and iron compete for absorption, so they must be taken at different times, ideally at least 2 hours apart. Calcium citrate in divided doses is the recommended form, and it should never be taken at the same time as your iron supplement.
How do I know if my multivitamin is working for recovery?
Regular lab checks are the only reliable way to confirm that your supplementation is preventing deficiencies. Tracking biochemical markers like ferritin and B12 over time gives you and your provider the data needed to adjust your regimen before symptoms appear.
Recommended
- Best Bariatric Multivitamins: Compare 15 Products by Price
- Bariatric Vitamin Guides for Bypass and Sleeve Patients
- Best Multivitamin After Gastric Bypass Surgery (2026)
- Bariatric Vitamin Deficiencies: What to Watch For
Find your bariatric multivitamin
Compare 15 products by price, surgery type, and iron content.
Compare 15 multivitamins